 This is an open access article distributed under the terms of the Creative Commons
Attribution License (
This is an open access article distributed under the terms of the Creative Commons
Attribution License (Setting the ground for possible cross-cultural comparisons, the importance of measuring mental health and well-being in Latin America is highlighted. Until now, research that has focused on studying mental health or well-being in Latin America—using valid and reliable versions of internationally well-known instruments—has been scarce. For example, some data has been obtained through surveys, such as those conducted by TNS Gallup in Argentina. A report published in 2011 showed that 8 out of 10 individuals claimed to be happy. In detail, younger people, women, and people who were in a relationship reported being the happiest groups (TNS Gallup, 2011). Castro Solano (2014) reviewed studies conducted in Latin American countries that centered on well-being, and found that three countries—Mexico, Argentina, and Peru—produced most of the research on this construct.
Furthermore, as Michaelson and colleagues have mentioned, there are other benefits of measuring population well-being, such as it allows one to assess change over time; to review and evaluate policy decisions, assess subgroup differences, identify future areas of need or opportunity, evaluate the potential impact of policy proposals, shape the content and delivery of policy, and inform targets of new policies according to population subgroups (Michaelson, Abdallah, Steuer, Thompson, & Marks, 2009). Traditionally, mental health has been characterized as the absence of psychological illness. However, it is clear that the absence of psychopathology does not imply the presence of mental health. The World Health Organization (WHO), since its inception, has defined mental health as a state of physical, mental, and social well-being, and not as merely the absence of disease (WHO, 1948, 2008). From a psychological perspective, mental health has been operationalized as psychological well-being, which has given rise to two traditions of study: hedonic and eudaimonic.
The hedonic conceptualization involves the study of happiness that focuses on positive emotions and life satisfaction (Diener, 2000; Diener, Emmons, Larsen, & Griffin, 1985; Pavot & Diener, 2008). Research in this field has demonstrated that a happy person lives longer, has better physical health, acquires more fulfilling jobs, and establishes good-quality personal relationships (Diener & Biswas-Diener, 2008). Moreover, positive emotions play an important role in physical health, social commitment, and success. Conversely, the eudaimonic approach retrieves concepts from the Greek tradition, understanding well-being as the result of virtuous activities and the meaning given to life. Toward the end of the 1980s, researchers on well-being, such as Carol Ryff, mentioned that happiness was more related to positive relationships as well as sense of purpose and meaning in life than to the experience of mere positive emotions. From this point of view, well-being means functioning well in life. Thus, eudaimonic happiness is related to personal growth and fulfillment at an individual level, and associated with commitment to goals and shared values at a societal level (Massimini & Delle Fave, 2000; Ryff, 1989). The eudaimonic perspective of well-being integrates Ryff’s theory of psychological well-being (Ryff, 1989), Antonovsky’s construct of sense of coherence (Antonovsky, 1988), the self-determination theory (Ryan & Deci, 2000, 2001), the concept of optimal selection (Csikszentmihalyi & Massimini, 1985), and Keyes’ social well-being construct (Keyes, 1998), among others.
Whereas the hedonic and eudaimonic traditions in the study of well-being have remained separated, recently, the unilateral approach to the study of well-being has been the subject of intense debates (Henderson & Knight, 2012; Kashdan, Biswas-Diener, & King, 2008; Waterman, 2008). Keyes (2002, 2005, 2007) tried to unify the study of hedonic and eudaimonic perspectives through the concept of flourishing, developing a specific instrument, the Mental Health Continuum (MHC), that comprehensively assesses the degree of positive mental health across the dimensions of emotional, social, and psychological well-being (Castro Solano, 2014). In line with the WHO definition of mental health, for this model, positive mental health is not simply the absence of mental disorders, but the presence of positive qualities; that is, high levels of emotional, psychological, and social well-being. Emotional well-being involves the presence of positive emotions and satisfaction with life (Diener, Suh, Lucas, & Smith, 1999). Psychological well-being comprises aspects of individuals’ psychological functioning (e.g., autonomy and a sense of personal growth; Ryff, 1989). Social well-being indicates how well an individual functions in their social life as a member of a larger society (e.g., social integration and social contribution; Keyes, 1998).
Keyes (2005, 2013) proposed a two continua model, and holds that mental illness and mental health are distinct, but related, dimensions. This mental health continuum consists of three levels of positive mental health: flourishing, moderate, and languishing mental health. Individuals with flourishing mental health are high in hedonic and positive functioning. By contrast, individuals with languishing mental health report both low hedonic and positive functioning. In sum, languishing is the absence of mental health. Languishing individuals are those who are stuck in life, feel empty, and lack interest and engagement. Individuals who are neither flourishing nor languishing are considered to have moderate mental health.
Regarding the importance of measuring population well-being, epidemiological studies using reports of flourishing—such as the MHC–SF—have shown that it is associated with superior physical, psychological, and psychosocial functioning (Keyes, 2005). By contrast, it was found that languishing is related to poor emotional health, frequent limitations of daily living, and more missed days of work (Keyes, 2002).
Given that many countries have adapted the MHC–SF, there is a considerable volume of evidence to support its utility, validity, and reliability. For example, factor analyses has confirmed the MHC–SF’s three-factor structure of emotional, psychological, and social well-being—found in earlier studies in the United States—in samples from South Korea (Lim, 2014), Italy (Petrillo, Capone, Caso, & Keyes, 2015), Poland (Karaś, Cieciuch, & Keyes, 2014), South Africa (Keyes, Wissing, Potgieter, Temane, Kruger, & van Rooy, 2008), and France (Salama-Younes & Ismaïl, 2011). Additionally, Joshanloo and colleagues investigated the factorial structure and invariance of the MHC–SF across cultural groups from three nations—the Netherlands, South Africa, and Iran—and the three dimensional structure was supported in all three groups (Joshanloo, Wissing, Khumalo, & Lamers, 2013). Furthermore, the MHC–SF has shown excellent internal consistency and criterion validity in adolescents and adults across different countries, including the United States, the Netherlands, Egypt, Italy, and South Africa, among other countries (Keyes, 2006; Keyes & Grzywacz, 2005; Keyes et al., 2008; Lamers, Westerhof, Bohlmeijer, ten Klooster, & Keyes, 2011; Petrillo et al., 2015; Salama-Younes & Ismaïl, 2011).
Petrillo et al. (2015) found that all the subscales of the MHC, on the one hand, have positively correlated with the corresponding aspects of functioning and well-being (e.g., satisfaction with life, positive emotions), showing convergent validity. On the other hand, the MHC’s subscales have negatively and moderately correlated with measures of mental illness (e.g., General Health Questionnaire 12 –GHQ–), indicating divergent validity. In addition, Lamers and colleagues reported test-retest reliability of the MHC–SF at four-time points over nine months, in a Dutch sample, using item response theory (Lamers et al., 2011). Similar results were found by Petrillo et al. (2015), who reported moderate test reliability.
Using exploratory and confirmatory factor analysis, most of the studies mentioned above have supported the two continua model of mental health (e.g., Lim, 2014; Karaś et al., 2014; Keyes, 2005; Keyes et al., 2008; Petrillo et al., 2015). The model with two distinct, but correlated (oblique), factors demonstrated a better set of fit coefficients than did other models (e.g., models with a single factor or two orthogonal factors). These findings confirm that mental health and mental illness are not the ends of one bipolar continuum, but two distinct and related dimensions.
Based on the aforementioned reasoning, the present research aimed to analyze the psychometric properties of the Mental Health Continuum–Short Form (MHC–SF; Keyes, 2005) in a sample of Argentinean adults. Both validity and reliability evidence were studied using a series of diverse statistical analyses, such as confirmatory factor analysis, cross-validation, factorial invariance, correlations with external criteria to assess convergent and divergent aspects, and internal consistency using Cronbach’s alphas. Also, this study aimed to obtain evidence for the two-continua model.
Method
Participants
A convenience sample of 1,300 Argentinean adults from the general population was studied. They were proportionally distributed by sex: 650 males (50%) and 650 females (50%). The mean age was 40.28 years old (SD = 13.59). The majority of the participants (83.5%; n = 1,088) lived in Buenos Aires, 3.9% (n = 51) lived in other provinces of Argentina, and only 3.5% (n = 46) reported living abroad temporarily. The remaining percentage (8.8%, n = 115) did not provide information regarding their residence. Regarding their education, 80.2% (n = 1,043) achieved higher educational degrees, such as college or postgraduate studies. The remaining 19.8% (n = 257) received at least an elementary and/or middle school education. Concerning their occupation, 57% (n = 741) reported being employed; 17.1% (n = 223) were self-employed; 9.7% (n = 127) were managers or employers; 3.8% (n = 49) were housekeepers or non-paid workers; and the remaining 12.1% (n = 157) were unemployed or did not work. Only 0.3% of the sample (n = 3) did not give any data regarding their occupation. When asked about their socioeconomic status, the highest percentage (73.1%, n = 951) described itself as belonging to the middle class, 16.6% (n = 216) to high or middle-high class, 10.2% (n = 132) to middle-low or lower class, and 0.1% (n = 1) did not provide any data.
Materials
Mental Health Continuum–Short Form (MHC–SF)
The original 14-item Mental Health Continuum–Short Form (MHC–SF; Keyes, 2005) was developed by Keyes in response to demands for a brief self-rating assessment tool that combined the three components of well-being: emotional, social, and psychological. The emotional well-being subscale –EWB– (three items) is defined in terms of positive affect/ satisfaction with life. Social well-being –SWB– is assessed with five items that represent each aspect of the model described by Keyes (1998): social contribution, social integration, social actualization, social acceptance, and social coherence. Finally, six items represent each of the dimensions of psychological well-being –PWB– as described in Ryff’s model (Ryff, 1989): self-acceptance, environmental mastery, positive relations with others, personal growth, autonomy, and purpose in life. Participants were required to respond to items on a 6-point Likert-type scale based on the experiences they had had over the last month (never, once or twice, about once a week, 2 or 3 times a week, almost every day, or every day). This response option was selected to provide a clear standard of mental health assessment and a categorization similar to the method used by the DSM (American Psychiatric Association, 2002, 2013) to assess a Major Depressive Episode (see the Results section for psychometric properties).
Satisfaction with Life Scale (SWLS)
The Satisfaction with Life Scale (SWLS; Diener et al., 1985; Pavot & Diener, 1993) was developed to obtain a measure of an individual’s general satisfaction with life. Evaluation of quality of life—according to self-perception—is measured on a cognitive–judgmental level. It comprises five items that are judged using a 7-point Likert-type scale, ranging from 1 (strongly disagree) to 7 (strongly agree). Cronbach’s alpha coefficient from the sample of this study was .87.
Positive and Negative Affect Scale (PANAS)
The Positive and Negative Affect Scale (PANAS; Watson, Clark, & Tellegen, 1988) was selected to measure positive (PA) and negative (NA) affect. PA reflects the extent to which a person feels enthusiastic and active, whereas NA refers to being alert, or to being sad, anxious, and depressed. Both dimensions are assessed by 14 descriptors each (a total of 28 items). Responses were given in a 5-point Likert-type scale ranging from 1 (low frequency) to 5 (high frequency). In this research, Cronbach’s alpha for PA was .76 and for NA was .85.
Meaning in Life Questionnaire (MLQ)
The Meaning in Life Questionnaire (MLQ; Steger, Frazier, Oishi, & Kaler, 2006; Argentinian adaptation: Góngora & Castro Solano, 2011) is an instrument to measure the presence of meaning in life. It refers to the extent to which people comprehend, make sense of, or see significance in their lives, accompanied by the degree to which they perceive themselves as having a purpose or mission in life. The adapted scale has two dimensions, presence of and search for, depending on whether people have goals and a purpose in life, or whether they believe they have to search for them. It comprises 10 items that are responded to on a 7-point Likert-type scale ranging from 1 (absolutely false) to 7 (absolutely true). The analysis of the adapted version has demonstrated adequate psychometric properties, such as reliability and convergent and divergent validity. In this study, Cronbach’s alpha for Presence was .88, and for Search was .87.
Well-Being Index (WBI)
The Well-Being Index (WBI; Cummins et al., 2001; translation: Tonon, 2012) contains 12 items of satisfaction that are answered on a 10-point Likert-type scale, where 1 = completely unsatisfied and 10 = completely satisfied. Each item corresponds to a quality of life domain, such as standard of living, health, achievement in life, relationships, safety, community connectedness, and future security. These domains are theoretically embedded as representing the first-level deconstruction of the global question: ‘How satisfied are you with your life as a whole? This measure not only includes subjective well-being, but also aspects of social life. Cronbach’s alpha for the total score was .88.
Self-Report Depression Scale for Research in the General Population (CES-D)
The Self-Report Depression Scale for Research in the General Population (CES-D; Radloff, 1977) is a short self-report scale designed to measure depressive symptomatology in the general population. The items of the scale are symptoms associated with depression that have been used in previously validated and longer scales. Participants are asked to rate on a 20-item scale how often, over the past week, they experienced symptoms associated with depression, such as restless sleep, poor appetite, and feeling lonely. Response options range from 0 to 3 for each item (0 = less than 1 day, 1 = 1–2 days, 2 = 3–4 days, 3 = 5–7 days). For the present study, Cronbach’s alpha reliability was .87.
Symptom Checklist-90-Revised (SCL-90-R)
The Symptom Checklist-90-Revised (SCL-90-R; Derogatis, 1977; Argentinian adaptation: Sanchez & Ledesma, 2009) is a 90-item checklist used to measure the nine sets of psychological symptoms: Somatization, Obsessive-compulsive, Interpersonal Sensitivity, Depression, Anxiety, Hostility, Phobic Anxiety, Paranoid Ideation, and Psychoticism. The SCL-90-R also contains a Global Severity Index (GSI), which is used to estimate the “general psychiatric status” of a patient. The SCL-90-R uses a 5-point scale (1 = no problem to 5 = very serious) to measure the extent to which they have experienced the listed symptoms in the last 7 days. Studies with the Argentinean adaptation of the checklist showed an adequate internal consistency for all of the scales (all alpha > .75) and also replicated the original factorial structure (e.g., Sanchez & Ledesma, 2009). Cronbach’s alpha coefficient from the sample of this study was .97.
Procedure
Regarding sampling method, it was a non-randomized sample. All participants were volunteers, and no incentives were provided for participation. Written informed consent was obtained before participation. Questionnaires were administered by psychology students from a university located in the city of Buenos Aires as part of their professional practices in research program. A senior researcher supervised their work.
The method used for translation of the MHC–SF was forward translation. Two researchers were involved in the translation process. Both have a Ph.D. in Psychology and a good command of the English language. They translated the MHC–SF independently and without any discussion. As judged by the translators, both versions did not differ noticeably. Afterwards, adjustments were conducted to ensure understandability, psychological equivalence, and the accuracy of the translation from English to Spanish.
Data were analyzed with SPSS 17.0 and EQS 6.2.
Results
Descriptive Statistics
First, univariate statistics were calculated for each item (Table 1). Most means had values around 3.5. Skewness and kurtosis values indicated univariate normal distribution for all items. However, a normalized estimate of Mardia’s coefficient of 51.20 indicated a non-normal multivariate distribution.
Table 1
MHC. Descriptive Univariate Statistics.
| Item | M | SD | Skewness | Kurtosis |
|---|---|---|---|---|
| Item 1 | 3.51 | 1.05 | -0.77 | 0.55 |
| Item 2 | 3.93 | 1.11 | -1.14 | 1.09 |
| Item 3 | 3.51 | 1.13 | -0.82 | 0.50 |
| Item 4 | 2.68 | 1.54 | -0.28 | -0.95 |
| Item 5 | 2.69 | 1.69 | -0.28 | -1.16 |
| Item 6 | 1.49 | 1.50 | 0.64 | -0.73 |
| Item 7 | 2.54 | 1.34 | -0.20 | -0.74 |
| Item 8 | 1.45 | 1.39 | 0.58 | -0.76 |
| Item 9 | 2.89 | 1.35 | -0.50 | -0.40 |
| Item 10 | 3.59 | 1.15 | -0.91 | 0.71 |
| Item 11 | 3.75 | 1.11 | -0.99 | 1.74 |
| Item 12 | 3.47 | 1.37 | -0.81 | -0.09 |
| Item 13 | 3.70 | 1.17 | -0.91 | 0.52 |
| Item 14 | 3.67 | 1.31 | -0.98 | 0.34 |
Confirmatory Factor Analysis
Confirmatory factor analysis (CFA) was run to ascertain the factor structure of the MHC–SF. Due to the categorical nature of the items (Likert-type scale), the estimation method used was robust Maximum Likelihood (ML), using the polychoric matrix. To assess model fit, different indexes of fit obtained by the robust method were examined: Satorra-Bentler, df, NFI (Normed-of-Fit Index), CFI (Comparative Fit Index), IFI (Incremental Fit Index), and RMSEA (Root Mean Square Error of Approximation). Different models were tested: (i) a single factor model with a unique measure of mental health, (ii) a two factor model were one latent dimension represented hedonic aspects of well-being –EWB– and the other dimension the eudaimonic aspects of well-being –both SWB and PWB–), (iii) a three factor with independent measures for EWB, PWB, and SWB as proposed by Keyes (2002, 2005), and (iv) a second order model were the three first order dimensions proposed by Keyes load in a general factor of mental health. Table 2 shows that the three-factor structure is the best-fitting model and it replicates the proposed latent structure of subjective well-being (see also Figure 1).
Table 2
Confirmatory Factor Models of Theories of the Latent Structure of the MHC–SF Items
| Model | Satorra-Bentler | df | IFI | NFI | CFI | RMSEA (IC 90%) |
|---|---|---|---|---|---|---|
| Single factor | 1678.5484 | 76 | .918 | .914 | .918 | .127 (.122 - .133) |
| Two factor | 1217.7772 | 74 | .941 | .938 | .942 | .109 (.104 - .114) |
| Three factor | 372.0408 | 71 | .977 | .973 | .977 | .065 (.059 - .070) |
| Second order (three factor) | 573.8704 | 67 | .974 | .971 | .974 | .076 (.071 - .082) |
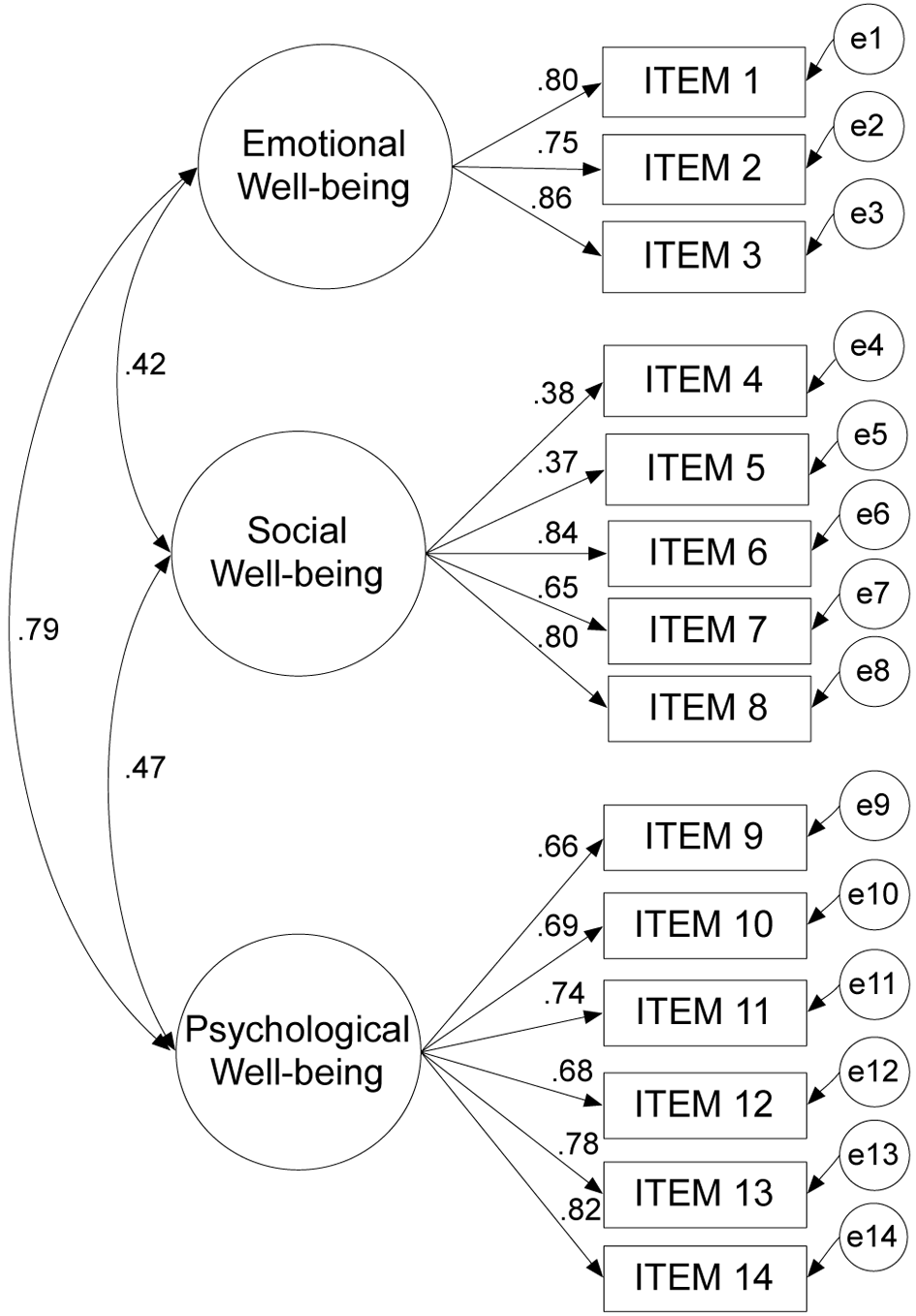
Figure 1
Confirmatory Factor Analysis of the MHC-SF (Three factor model).
Cross-Validation
Next, cross-validation analyses were conducted to test whether the Three factor model fit prevailed in samples differentiated by sex and age. The sample was first divided in two: females (n = 650) and males (n = 650). As presented in Table 3, model fit indices showed excellent fit in both samples. Then, the main sample was divided into two age groups: the first sample consisted of individuals between 18 and 40 years old (n = 678), and the second group consisted of those whose ages ranged from 41 to 86 years (n = 622). Again, model fit was assessed using the robust method for ML. Indices of fit showed the appropriateness of the measurement model (Table 3).
Table 3
Cross-Validation: Model Fit by Sex and Age.
| Sample | CFI | NFI | IFI | RMSEA (IC 90%) |
|---|---|---|---|---|
| Sex | ||||
| Males | .979 | .971 | .979 | .064 (.056 - .072) |
| Females | .975 | .966 | .975 | .064 (.056 - .072) |
| Age | ||||
| 18 to 40 years old | .976 | .967 | .976 | .064 (.056 - .072) |
| 41 to 86 years old | .977 | .969 | .977 | .067 (.058 - .075) |
Factorial Invariance
Additionally, hierarchical models with constraints were studied in order to analyse factorial invariance. This was done twice: first, to test invariance between the female and male samples, and second, to test invariance between younger and older adults (18 to 40 years old vs. 41 to 86 years old).
Initially, model fit was tested without constraints (MODEL 1) for both male and female samples. Both CFI and RMSEA values were adequate (see Table 4). A second model (MODEL 2) imposed constraints in all factor loadings. Again, the model’s estimates fit the data at an acceptable level. The third and last model tested (MODEL 3) also imposed constraints in covariances. Data provided an adequate fit for this model.
Table 4
MHC-SF. Factorial Invariance Across Sex (Males vs. Females).
| Model | Satorra-Bentler | df | CFI | RMSEA (IC90%) | Model comparison | Δ S-B | Δ df | p | Δ CFI |
|---|---|---|---|---|---|---|---|---|---|
| Model 1 No constraints |
541.8734 | 148 | .977 | .064 (.058 - .070) | - | - | - | - | - |
| Model 2 Factor loadings constrained |
563.2271 | 159 | .976 | .063 (.057 - .068) | 2 vs 1 | 16.27 | 11 | .131 | .001 |
| Model 3 Factor loadings and covariances constrained |
567.5102 | 162 | .976 | .062 (.057 - .068) | 3 vs 1 | 20.55 | 14 | .113 | 0 |
Table 4 also shows values for model comparison. Neither the difference in the Satorra-Bentler scaled statistic (ΔS-B) corresponding to the comparison of MODEL 1 versus MODEL 2, nor the one for the stricter model (MODEL 3) that also imposed constraints in covariances, showed a significant change in the S-B scaled statistic (p > .05). Moreover, the delta CFI indicated no change in fit (invariance) among the studied models.
When testing for factorial invariances in age-compared groups, the same procedures were run. First, a model with no constraints was tested (MODEL 1), then factor loadings were imposed (MODEL 2), and finally, covariances were constrained (MODEL 3). CFI and RMSEA values were adequate in all models. Model comparison showed no statistically significant difference in the Satorra-Bentler scaled statistic between MODEL 1 and 2, nor between MODEL 1 and MODEL 3. No changes were found in the CFI, either (Table 5).
Table 5
MHC-SF. Factorial Invariance Across Two Age Groups (18- to 40-yrs vs. 41- to 86-yrs).
| Model | Satorra-Bentler | df | CFI | RMSEA (IC90%) | Model comparison | Δ S-B | Δ df | P | Δ CFI |
|---|---|---|---|---|---|---|---|---|---|
| Model 1 No constraints |
556.3623 | 148 | .976 | .065 (.059 - .071) | - | - | - | - | - |
| Model 2 Factor loadings constrained |
573.7543 | 159 | .976 | .063 (.058 - .069) | 2 vs 1 | 10.16 | 11 | .515 | 0 |
| Model 3 Factor loadings and covariances constrained |
576.6922 | 162 | .976 | .063 (.057 - .068) | 3 vs 1 | 10.05 | 14 | .757 | 0 |
Internal Consistency
Table 6 summarizes the descriptive and correlational statistics obtained on the total MHC–SF scale and its three subscales. The highest means were obtained for emotional and psychological well-being, whereas the lowest value was obtained for social well-being. These results are consistent with those found in previous research conducted in other countries (e.g., Keyes et al., 2008; Lamers et al., 2011). Also, the EWB and PWB subscales have a stronger association with each other than they do with SWB.
Table 6
Descriptive Statistics and Correlations of the MHC–SF Subscales and Total MHC–SF Score
| MHC–SF | M | SD | Correlations
|
|||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |||
| 1. Emotional well-being (EWB) | 3.65 | .94 | – | |||
| 2. Psychological well-being (PWB) | 3.51 | .94 | .62** | – | ||
| 3. Social well-being (SWB) | 2.17 | 1.08 | .45** | .51** | – | |
| 4. Total MHC–SF | 3.06 | .83 | .73** | .89** | .84** | – |
**p < .01.
Cronbach’s alpha coefficients were calculated to study internal consistency. The alpha coefficients for the MHC–SF scales were satisfactory. Reliability values above .70 are referred to as acceptable, and above .80 as high (Kline, 2000; Nunnally & Berstein, 1995). The total MHC–SF scale yielded a high internal consistency (alpha = .89). The PWB subscale had the next highest measure of internal consistency (alpha = .84), followed by the EWB subscale (alpha = .82), and finally, the SWB subscale (alpha = 0.78).
Convergent and Divergent Validity
Three hypotheses were formulated according to Keyes’ conceptualization (Keyes, 2002). It was first hypothesized that the Emotional Well-Being subscale (EWB) would positively correlate with measures of positive affect and satisfaction with life. Second, it was hypothesized that the Psychological Well-Being subscale (PWB) would have a positive correlation with measures of positive functioning (e.g., tests to assess purpose in life). Finally, it was postulated that the Social Well-Being subscale (SWB) would have a positive association with measures that suggest well-being in different aspects of social life. Moreover, it was also hypothesized that the total score of the MHC–SF would negatively correlate with measures of mental illness and negative affect. In order to test these hypotheses, Spearman’s correlations were calculated among the MHC–SF and different measures of well-being and functioning.
The total score of the MHC–SF scale generally revealed a consistent pattern of correlations with the criterion measures. As expected, the EWB positively correlated with satisfaction with life (SWLS) and the PANAS PA scale. Also, the PWB showed a positive association with the presence of meaning in life (MLQ). Finally, the SWB subscale had a positive and strong correlation with the WBI score, which is mainly considered a measure of social well-being. Furthermore, the MHC–SF total score and its subscales negatively correlated with the PANAS NA, the search for meaning in life (MLQ), and a measure of depression symptoms (CES-D). Most of the correlations obtained had moderate (rs ≥ .30) to large (rs ≥ .50) effect sizes (Cohen, 1992; see Table 7).
Table 7
MHC-SF. Bivariate Correlations with Validation Measures
| Validity measure | Emotional well-being (EWB) |
Psychological well-being (PWB) |
Social well-being (SWB) |
Total MHC–SF |
|---|---|---|---|---|
| PANAS PA (positive affect) | .47** | .30** | .43** | .44** |
| PANAS NA (negative affect) | -.31** | -.21** | -.31** | -.33** |
| SWLS | .56** | .54** | .35** | .54** |
| Presence of meaning in life (MLQ) | .48** | .49** | .23** | .46** |
| Search for meaning in life (MLQ) | -.23** | -.17** | -.32** | -.14** |
| WBI | .52** | .39** | .56** | .55** |
| CES-D | -.49** | -.38** | -.19** | -.37** |
**p < .01.
Evidence of Two-Continua Model
The two-continua model suggests that mental health and mental illness constitute two distinguishable but related factors and that they are not two sides of the same continuum. In order to obtain evidence for the two-continua model, two factor analyses (exploratory and confirmatory) were performed using the MHC-SF and SCL-90-R subscales, which assess psychopathological symptoms.
Firstly, for the exploratory factor analysis a forced two factor solution with Varimax rotation was performed. It was expected that the subscales of SCL-90-R (indicators of mental illness) would load in one factor and the subscales of MHC-SF (indicators of well-being) in another one. The results showed the anticipated two separated factors: one with high loadings of all of MHC-SF’s subscales and the other with high loadings of all of the SCL-90-R’s subscales (Bartlett’s sphericity test = 6491.44, p < .001, KMO index = .97). The explained variance for this solution was 71% (see Table 8).
Table 8
Exploratory Factor Analysis With Two Factors: Mental Health and Mental Illness
| Subscale | Factor 1 Mental health (MHC) |
Factor 2 Mental illness (SCL-90-R) |
|---|---|---|
| Social well-being (MHC) | .83 | |
| Emotional well-being (MHC) | .79 | |
| Psychological well-being (MHC) | .79 | |
| Psychoticism (SCL) | .89 | |
| Anxiety (SCL) | .88 | |
| Interpersonal sensitivity (SCL) | .83 | |
| Depression (SCL) | .83 | |
| Somatizations (SCL) | .82 | |
| Paranoid ideation (SCL) | .80 | |
| Phobic anxiety (SCL) | .79 | |
| Obsessions and compulsions (SCL) | .77 | |
| Hostility (SCL) | .76 |
Next, three models were studied using confirmatory factor analysis. The first one included one single factor with all the subscales from SCL-90-R and from MHC-SF. The second model proposed a structure of two orthogonal factors (first with the subscales from SCL-90-R, as the indicators of mental illness and second one with the subscales from MHC-SF as the indicators of mental health). The third model represented the two-continua model of two separated but correlated factors.
The two-continua model is the best-fitting data model to these data, suggesting that the correlated two-factor model was the most tenable model of the structure of mental health and illness. RMSEA was right on the expected limits (Kline, 2000) but lower than those obtained in the other models. The correlation between the latent factors of mental illness and mental health was -.50 which indicated, as expected, a moderate correlation of two aspects which are related but are not the same construct. These results confirm the two-continua model (see Table 9).
Table 9
Confirmatory Factor Models -Verification of the Structure of Mental Health and Mental Illness.
| Model | Satorra-Bentler | Df | IFI | NFI | CFI | RMSEA (IC 90%) |
|---|---|---|---|---|---|---|
| Single factor | 538.3717 | 53 | .837 | .822 | .836 | .113 (.105 - .122) |
| Two orthogonal factor | 368.4632 | 52 | .894 | .878 | .893 | .093 (.084 - .101) |
| Two correlated factor | 284.2207 | 51 | .922 | .906 | .921 | .080 (.071 - .089) |
Discussion
The Mental Health Continuum, or MHC, represents a clinical approach to the continuous assessment and categorical diagnosis of states of positive mental health (Keyes, 1998, 2002; Keyes et al., 2008). The short form of the MHC scale, consisting of 14 items, is one of the instruments to assess well-being most widely used internationally. For this reason, the main objective of this study was to validate the MHC–SF within an Argentinian population. The current findings confirm that the Argentinian MHC–SF is a valid and reliable instrument that can be used for assessing well-being within the Argentinean population.
In this study, robust evidence of construct validity was found for a three-factor structure of emotional, psychological, and social well-being. The same structure was found in earlier studies in the United States, and more recently, in samples from South Korea (Lim, 2014), Italy (Petrillo et al., 2015), Poland (Karaś et al., 2014), South Africa (Keyes et al., 2008), and France (Salama-Younes & Ismaïl, 2011), among others. Although Item 4 and 5 had lower factor loading in comparison with other items, they were retained to maintain the original number of items and desirable for each factor. Considering the sample size used, some authors argue that .32 can be acceptable because it would be equivalent to approximately 10% of the variance explained (Tabachnick & Fidell, 2001).
In this research, the model fits well not only in the main sample, but also in the cross- validation study, indicating that the fit prevailed in the female and in the male sample. Moreover, excellent fit was also found when the sample was split into a group of younger and older adults. Additionally, several tests of factorial invariance performed in the mentioned samples showed that model fit was appropriate even when constraints in loadings and covariances were imposed. Data supports the adequacy of the three-dimensional model of the MHC for Argentinean adults, regardless of sex or age.
Furthermore, the MHC–SF has shown excellent internal consistency and criterion validity because it positively correlated with measures of well-being and was negatively associated with measures of mental illness. The data support the hypotheses on convergent and divergent validity. These results are consistent with the two continua model, which has proposed that mental illness and mental health are distinct, but related, dimensions (Keyes, 2005). Also, evidence for this model was obtained using a measure of psychopathological symptoms (SCL-90-R).
In the studied sample, Items 6 and 8 showed mean values lower than expected. Although this results are not uncommon as similar results were obtained in samples from other countries (e.g. Joshanloo et al., 2013), their interpretation in light of local aspects is not out of place as these items are related to social factors. It is possible that this is related to the insatisfaction Argentinians have with some aspects related to society, especially regarding security. This aspect can also be observed in the differential association among presence of meaning in life (MLQ) and MHC-SF’s subscales which were strong with emotional well-being and psychological well-being but weak with social well-being.
Future studies may use this instrument to obtain estimates of the prevalence of mental health categories in Argentina (i.e., determining the percentage of flourishing, languishing, and moderately mentally healthy individuals). In addition to the importance of having an instrument to assess well-being in Argentina, the psychometric evidence obtained for the three-factor structure allows cross-cultural comparisons and prevents possible variations in prevalence rates due to different versions of the instruments used. For example, Hone, Jarden, Schofield, and Duncan (2014) found important variation in the prevalence of flourishing among 10,009 adults in New Zealand, based on the use of four different operationalizations: Huppert and So (2013; 24%), Keyes (39%), Diener et al. (41%), and Seligman et al. (47%).
Some of the limitations of the present study are related to the use of self- reported data and the utilization of convenience samples. Future studies should employ non-self-report assessments and more representative samples. Finally, more research should be done to (a) investigate the predictive validity of the MHC–SF in terms of health and illness outcomes and work productivity, among other important public health outcomes (Karaś et al., 2014), and (b) explore the levels of well-being in specific groups of people (e.g., teachers; Petrillo et al., 2015) in countries like Argentina.