 This is an open access article distributed under the terms of the Creative Commons
Attribution License (
This is an open access article distributed under the terms of the Creative Commons
Attribution License (Employees are constantly exposed to work interruptions, which are inevitable in many work environments. Work interruptions interfere with completing important job tasks, leading to a loss of efficiency and postponement of an activity (Zijlstra, Roe, Leonora, & Krediet, 1999). On a related note, the rise of modern technology available twenty-four hours a day via emails, laptops or smart phones hinders recovery from work (Boswell & Olson-Buchanan, 2007). Users’ attention is disrupted at work when users respond to instant messaging via smart phones (Rennecker & Godwin, 2005). Access to smart phones outside of working hours has been associated with fatigue and sleep problems (Derks & Bakker, 2014).
How individuals interpret such demands is crucially important as interruptions can awaken ruminative thinking over work issues, and hence impair post work recovery. Prior research has demonstrated that factors such as positive work values were positively related to job satisfaction, negatively related to physical symptoms, and moderated the relationship between work stressors and level of wellbeing (Lu, Kao, Siu, & Lu, 2011). Thus, investigating employees’ work beliefs on wellbeing could provide important practical recommendations on how to enhance employees’ motivation and performance. Prior research has demonstrated that beliefs in delay of gratification, and in self-reliance were predictors of job performance and task efficiency among employees in a financial management organization (Miller, Woehr, & Hudspeth, 2002).
The present study aims to increase our understanding of the relationship between work interruptions, work beliefs and wellbeing. Specifically, we draw on Lazarus’ (1966) cognitive theory of stress and the Effort-Recovery Model (ERM; Meijman & Mulder, 1998) to examine whether employees holding particular work beliefs benefit more on psychological and physiological components of wellbeing. Following Lazarus’ stress approach, which consists of the appraisal of resources and coping options with an indirect or direct effect on stress, we examine work beliefs as a moderator between work interruptions and wellbeing. Along similar lines, psychological and physiological costs are discussed in the ERM (Meijman & Mulder, 1998) as the product of work effort and insufficient recovery. Higher levels of work effort, according to the Effort Recovery theory, can increase the prevalence of chronic fatigue and sleep deprivation (Åkerstedt, 2006; Härmä, 2006). According to ERM, physiological unwinding is an important aspect of the recovery process. ERM underscores the association between the amount of effort put in at work and chronic overwork reactions (i.e., fatigue, physical health complaints and impaired sleep). Chronic overwork occurs when employees are exposed to constant workload followed by inadequate relaxation from work (Meijman & Mulder, 1998).
Hassall, Muller, and Hassall (2005) showed that improved wellbeing was pronounced among employees endorsing positive beliefs in the values of hard work and work regard. In line with this, we examine whether work beliefs can moderate exposure to job demands such as work interruptions. In the following sections, we discuss the rationale.
Cognitive Theory of Stress and Work Beliefs
Lazarus’ (1966) cognitive theory of stress, posits that cognitive beliefs of demands and resistance resources are important determinants of stress. According to the transactional model of stress and coping (Lazarus & Folkman, 1984), a threatening event, which is interpreted by the person and the environment transactions, affects the person’s reactions. Lazarus’ cognitive theory of stress has been further developed to a meta-theoretical approach with focus on individuals’ coping processes (Lazarus, 1991), and it posits that emotional processes are composed of antecedents, immediate effects of stress and mediating processes. Antecedents refer to stressful experiences. Immediate effects refer to physiological reactivity, and affect due to stress exposure. Mediating processes refer to individuals’ cognitive appraisals of an event as stressful or positive (primary appraisals), and secondary appraisals based on evaluation of individuals’ coping efforts which have indirect effects on affect and physiological reactivity, and long-term effects on psychological wellbeing and somatic symptoms (Lazarus, 1991; Lazarus & Cohen, 1977). Cognitive appraisals refer to an individual’s evaluation of coping options such as competence, energy and support in order to encounter demands. While situations that are appraised as easy do not set off an alarm reaction, more harmful or threatening situations may lead to the onset of a stress reaction (Lazarus & Folkman, 1987).
This study explores how work interruptions and beliefs affect physical and psychological wellbeing. Our reasoning is that work beliefs would play a salient role in the relationship between work interruptions and physical and psychological wellbeing.
Work Ethic and Beliefs
Work beliefs have been linked to work ethic (Miller et al., 2002; Weber, 1976). Furnham (1990) refers to work ethic as comprised of beliefs in hard work, leisure beliefs, religious and moral beliefs, independence from others and asceticism beliefs. Protestant work ethic (PWE) has been associated with certain types of work attitudes and behaviour e.g. delay of gratification, high responsibility for personal matters and increased interest towards work (Mirels & Garrett, 1971). Mudrack (1997) defined four work beliefs related to hard work, asceticism, and negative views of others and anti-leisure. It has been argued that the work ethic beliefs are part of a robust belief system (Furnham & Rose, 1987).
Furnham and Rose (1987) refer to leisure ethics as time for recreation rather than as human fulfilment, thus suggesting two things: first, work is accepted as a way of earning money. Second, the work time is meaningful but individuals have the choice to pursue activities during leisure time (Furnham & Rose, 1987). In accordance with Furnham and Rose’s (1987) assertion, leisure ethics were negatively associated with work ethic. On one hand, anti-work beliefs such as “work is boring and stressful” were not correlated with a strong work ethic. On the other hand, PWE was positively related to others factors such as delay of gratification, economic beliefs and locus of control. Anti-work beliefs, welfare ethic, wealth ethic e.g. “one works to live” and leisure beliefs e.g. “leisure is good for people” overlapped and were all positively associated with each other (Furnham & Rose, 1987). Because of this strong relationship, beliefs have been an important measure of perceived attitude to work.
Effort Recovery Model
Work recovery has a prominent role in occupational stress models. In the ERM (Meijman & Mulder, 1998), for example, recovery during off job hours is considered critical, and can lead to increased motivation, and work engagement as well as reducing stress. Studies have shown that employees exhausted due to overtime that takes place outside normal work hours, experience cognitive decline, reduced physical vigour, cognitive liveliness and recovery (Oerlemans & Baker, 2014), and are disengaged from work (Demerouti, Mostert, & Bakker, 2010).
The ERM states the importance of psycho-physiological systems to return to a baseline, and consequently the replenishment of resources. Otherwise, employees are forced to put extra effort to compensate for their reduced vigour, which consequently may result in chronic load reactions such as fatigue and sleep problems (van Hooff et al., 2005). In line with this reasoning, individuals with insufficient recovery experienced chronic stress and health impairments (Geurts & Sonnentag, 2006), and slow recovery after work was found to be related to elevated cortisol levels and various health problems (Ganster, Fox, & Dwyer, 2001; Rydstedt, Cropley, Devereux, & Michalianou, 2008).
Work Interruptions, Work Beliefs and Wellbeing
Research has shown that work interruptions and strongly held beliefs in hard work and self-reliance can help employees detach from work. Employees who possessed such work beliefs coupled with positive appraisal of work interruptions reported increased levels of detachment from work (Zoupanou, Cropley, & Rydstedt, 2013).
Hassall and colleagues (2005) demonstrated that low psychological distress and increased wellbeing were noticeable among employed and unemployed adults endorsing strong beliefs in hard work, holding regard for work (i.e. doing a good job) labelled Work Regard belief and negative attitude to leisure. One interpretation of this was that work was valued as meaningful by the employed, in terms of, for example, self-esteem and financial advantages. These workers with a strong belief in hard work also did not have regard for the value of leisure, thus generating a so called anti-leisure belief: they worked hard and kept themselves busy and this was perceived as a means of improving their financial state and confidence. Hassall et al. (2005) also found that unemployed participants associated a belief in hard work with improved wellbeing (Hassall et al., 2005). They committed themselves to hard work leading to increase in self-esteem and wellbeing There is still, however, limited evidence regarding whether work interruptions are linked to this relationship between work beliefs and wellbeing. The results of a qualitative study on work interruptions highlighted work values as an important theme of work ideology among managers (Zoupanou, 2015). Core work beliefs which encapsulated beliefs in centrality of work and acceptance towards work interruptions were integrated into a clear philosophical framework “interruptions are part of the job” (Zoupanou, 2015). Furthermore, a study focused on the moderating role of work beliefs on work interruptions and work rumination (Zoupanou et al., 2013), found that negative belief in leisure and belief in delay of gratification served as moderating factors on the relationship between appraisal of work interruptions and elevated problem solving in particular. Employees who held lower beliefs in leisure time and in delay of gratification coupled with negative appraisal of work interruptions reported elevated pondering over work problems (Zoupanou et al., 2013). However, employees who endorsed lower belief in the importance of work coupled with a negative appraisal of work interruptions reported limited pondering over solving work problems (Zoupanou et al., 2013). In the present study we attempt to test the possible effects of work values on wellbeing in relation to the impact of work interruptions, and propose the following hypotheses:
Hypothesis 1: Positive work beliefs will be associated with general health and wellbeing, as well as to lower levels of physical symptoms.
Hypothesis 2: Employees’ work beliefs will moderate the relationship between work interruptions, general health and wellbeing, so that it is better for employees who endorsed high levels of positive work beliefs.
Hypothesis 3: Work beliefs will moderate the relationship between the appraisal of work interruptions and physical symptoms, and this relationship will be stronger among employees who endorsed high levels of positive work beliefs.
Methods
Ethics Statement
The current study was a secondary data analysis collected for the purposes of a prior study (Zoupanou et al., 2013), and did not require formal ethics procedure (Grinyer, 2009). It was carried out in accordance with ethical guidelines of the University of Surrey and the British Psychological Society. Issues of confidentiality and anonymity (of the data) were guaranteed. Participants were asked to give written consent to participate and could withdraw from the study if they wished.
Participants
The study utilised a data set from the study ‘Recovery after work’ (Zoupanou et al., 2013), where the same individuals who had participated in self-report questionnaires on work ethic and on work interruptions measures were included in the present analyses. The original sample consisted of 310 white-collar employees particularly from the private business sector, recruited from a range of organizations: 73% worked in customer marketing services, 20% held managerial positions and 7% worked in the accounting and executive sector; 50% were males (N = 155) with a mean age of 35.2 years (SD = 10.7). The females (N = 155) had a mean age of 32 years (SD = 10.5). All employees worked full time with a mean of 40.6 (SD = 14.4) working hours per week.
Instruments
Stressors Question
This included the question “In general how stressful do you find your job?” (Smith, Johal, Wadsworth, Smith, & Peters, 2000). This was a self-evaluative question previously used in the Bristol Stress study. The response format of the question utilized a five-point scale (1 = Not at all stressful to 5 = extremely stressful).
Interruption Questionnaire
This measure comprised 13 items (Duggan, 2009). Due to content validity, two conceptually inconsistent items were deleted from the measure. A four-point scale was utilised (1 = strongly disagree; 4 = Strongly Agree). Items included “I find being interrupted at work is a welcome distraction”, “It does not trouble me to leave work unfinished at the end of the day”, “Interruptions can be a welcome break”, “Interruptions reduce boredom”. Principal component analysis revealed the presence of two components with eigen values exceeding 1, and accounted for 55.16% of the total variance. Seven items were loaded on Factor 1 (factor loading of .3 or greater on only one factor) which was termed negative interruption. Three items loaded on Factor 2, which was labelled positive interruption. The Cronbach’s alpha values for the negative interruption factor was 0.85 (M = 16.44, SD = 3.12), and for the positive interruption 0.78 (M = 10.79, SD = 1.57). The correlation between the two factors was moderate (r = .35) (Cohen, 1992).
Multidimensional Work Ethic Profile Measure (MWEP)
The MWEP (Miller et al., 2002) originally comprises 65 items rated on a Likert scale (1 = strongly agree; 5 = strongly disagree), a lower overall score indicated greater belief in work. The MWEP supported seven dimensions: Centrality of Work, Delay of Gratification, Hard Work, Leisure, Morality/Ethics (e.g. “one should always take responsibility for one’s actions”, “stealing is all right as long as you do not get caught”, “one should not pass judgement until one has heard all of the facts”), Self-Reliance and Wasted Time. The internal consistency (Cronbach’s alpha) of the factors was good: Wasted Time (α = .72, 7 items), Delay of Gratification (α = .82, 7 items), Centrality of Work (α = .82, 10 items), Hard Work (α = .86, 10 items), Leisure (α = .89, 10 items), Morality/Ethics (α = .78, 10 items). The Morality/Ethics measure was recoded on a Likert scale (5 = strongly agree; 1 = strongly disagree).
The Pennebaker Inventory of Limbic Languidness (PILL)
The short version of PILL was used to assess 21 items of physical symptoms (e.g., ‘your mouth became dry’, ‘your muscles felt tight’). Participants rated each of the symptoms on a five-point scale (1 = never; 5 = very often) to indicate how often they had experienced any of the symptoms during the past month. In the present study the Cronbach’s alpha value coefficient was α = .89.
General Health Questionnaire (GHQ)
Health and wellbeing was assessed using the 12 item version of the GHQ (Goldberg & Hillier, 1979). The validity of the GHQ-12 has been assessed in 15 different countries (Goldberg et al., 1997; Liang et al., 2016; Wang & Lin, 2011). In the current study we support the one factor model based on the argument that the GHQ-12 was initially designed as a unidimensional scale which allowed the analysis to keep its simplicity. A health survey for England (Hankins, 2008) also found the GHQ-12 as a unidimensional model due to correlation errors on negative wording items. In the present study participants were asked to report recent feelings in relation to anxiety, depression, self-esteem and cognitive processing. Participants had to respond, for example, to the question “How they have been feeling over the past few weeks”. Items were rated using a four-point scale (1 = better than usual; 4 = much less than usual). The scale had high internal reliability with а coefficient α between 0.82 and 0.86 (Politi, Piccinelli, & Wilkinson, 1994; Sriram, Chandrashekar, Isaac, & Shanmugham, 1989; Winefield, Goldney, Winefield, & Tiggemann, 1989). In the present study the Cronbach’s alpha value coefficient for the scale was α = .86.
Results
Correlations, means and standard deviations for all variables used in the present study are presented in Table 1. As further shown in Table 1, GHQ was positively related to beliefs in the importance of centrality of work and negatively related to beliefs in leisure. GHQ was uncorrelated with self-reliance, morality, hard work, wasted time, delay of gratification age. GHQ significantly correlated with stressful job.
Table 1
Pearson’s r Correlation Coefficients Between Demographic Variables and Measures of Wellbeing (N = 310)
| Variable | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. NI | 2.35 | 0.44 | - | ||||||||||||
| 2. PI | 3.60 | 0.52 | .38** | - | |||||||||||
| 3. PILL | 1.59 | 0.49 | .27** | .08 | - | ||||||||||
| 4. GHQ | 1.93 | 0.44 | .24** | -.04 | .54** | - | |||||||||
| 5. Self Reliance | 2.64 | 0.59 | -.18** | .00 | -.14* | -.00 | - | ||||||||
| 6. Morality | 3.09 | 0.97 | -.05 | .04 | .02 | -.01 | -.20** | - | |||||||
| 7. Leisure | 2.51 | 0.63 | -.16** | .18** | -.27** | -.22** | .20** | .01 | - | ||||||
| 8. Hard Work | 2.44 | 0.60 | .00 | .05 | -.04 | .10 | .43** | -.30** | -.00 | - | |||||
| 9. COW | 2.35 | 0.59 | .04 | -.04 | .08 | .13* | .15** | -.24** | -.44** | .40** | - | ||||
| 10. Wasted Time | 2.37 | 0.54 | -.15** | -.23** | .03 | .04 | .26** | -.32** | -.07 | .47** | .42** | - | |||
| 11. DOG | 2.71 | 0.68 | - .09 | -.11 | .13* | .08 | .28** | -.14* | -.05 | .33** | .23** | .30** | - | ||
| 12. Age | 34 | 11 | .00 | .22** | -.17** | -.02 | -.00 | .04 | .29** | .17** | .00 | -.07 | .04 | - | |
| 13. Stressful job? | 2.78 | 0.85 | .25** | .10 | .26** | .32** | .05 | .08 | -.12* | .08 | .22** | .03 | .17** | .03 | - |
Note. NI = Negative Interruption; PI = Positive Interruption; PILL = Physical Illness Symptoms; GHQ = General Health Questionnaire; COW = Centrality of Work; DOG = Delay of Gratification; Stressful Job = In general, how stressful do you find your job?
*p < .05. **p < .01.
Table 1 also shows a negative relation between physical symptoms and beliefs in self-reliance (r = -.14) and leisure (r = -.27) and positive relation between physical symptoms and delay of gratification (r = .13). Negative interruption related negatively to self-reliance (r = -.18), leisure beliefs (r = -.16), wasted time (r = -.15). Negative interruption related positively to general health and physical symptoms. Positive interruption was positively correlated with leisure (r = .18) and negatively correlated with the importance of not wasting time (r = -.23)
Moderating Effects of Work Beliefs
Moderated regression analysis (Baron & Kenny, 1986) was utilised to test the interaction effects of types of work belief on wellbeing and physical illness symptoms. We computed a two-step hierarchical multiple regression analysis (Baron & Kenny, 1986), using the centred variables of positive interruption, negative interruption and each dimension of work beliefs. The two dimensions of work interruptions and each dimension of work beliefs were introduced in Step 1. Interactions between work beliefs and the two dimensions of work interruptions with general health and psychosomatic symptoms were entered in Step 2. Two-way interactions between each dimension of work interruption and the seven dimensions of work beliefs assessed whether work beliefs moderated the relationship of negative and positive work interruption with general health and wellbeing, and then whether such work beliefs moderated the relationship of positive and negative work interruption with physical symptoms. Interaction terms were composed of the product of the variables, and these were centred to avoid problems of multi-collinearity. Evidence of moderation would be apparent if there was a statistically significant change in the variance accounted for by GHQ and psychosomatic symptoms with the introduction of the interaction terms (Cohen & Cohen, 1983).
Table 2 reports standardized coefficients for the hierarchical regression analyses predicting GHQ and psychosomatic symptoms. There was a significant positive correlation between psychosomatic symptoms and negative interruption (r = .37, p < .01). After centering the means for the interaction term, inspection of moderators of the relationship between negative interruption and work beliefs showed that none of the interaction terms was significant for the prediction of psychosomatic symptoms (Table 2). The correlation between negative interruption and GHQ was small but significant (r = .24, p < .01). However, interaction terms between negative interruption and work beliefs did not make any meaningful contributions to the prediction of GHQ (Table 2).
Table 2
Results of Regression Analysis of Negative, Positive Interruption and Work Beliefs on Psychosomatic Symptoms and General Health
| Dependent Variable | Psychosomatic Symptoms
|
General Health
|
||||
|---|---|---|---|---|---|---|
| B | SE | ß | B | SE | ß | |
| Step 1 | ||||||
| Negative Interruption | 0.25 | 0.06 | 0.23* | 0.20 | 0.05 | 0.21* |
| Leisure | -0.18 | 0.04 | -0.23 | -0.13 | 0.04 | -0.19* |
| Step 2 | ||||||
| Negative Interruption x leisure | -0.03 | 0.08 | -0.02 | 0.01 | 0.08 | 0.00 |
| Step 1 | ||||||
| Negative Interruption | 0.28 | 0.06 | 0.25* | 0.24 | 0.05 | 0.24* |
| Self reliance | -0.07 | 0.04 | -0.08 | 0.03 | 0.04 | 0.04 |
| Step 2 | ||||||
| Negative Interruption x Self Reliance | -0.16 | 0.09 | -0.10 | -0.05 | 0.08 | -0.03 |
| Step 1 | ||||||
| Negative Interruption | 0.29 | 0.06 | 0.27* | 0.23 | 0.05 | 0.24* |
| Hard work | -0.03 | 0.04 | -0.04 | 0.07 | 0.04 | 0.10 |
| Step 2 | ||||||
| Negative Interruption x Hard Work | -0.07 | 0.10 | -0.04 | 0.00 | 0.09 | 0.00 |
| Step 1 | ||||||
| Negative Interruption | 0.31 | 0.06 | 0.28* | 0.25 | 0.05 | 0.25* |
| Delay of Gratification | 0.11 | 0.04 | 0.16* | 0.07 | 0.03 | 0.11** |
| Step 2 | ||||||
| Negative Interruption x DOG | 0.04 | 0.08 | 0.02 | 0.11 | 0.07 | 0.08 |
| Step 1 | ||||||
| Negative Interruption | 0.29 | 0.06 | 0.27* | 0.23 | 0.05 | 0.24* |
| Morality/Ethic | 0.02 | 0.03 | 0.03 | 0.00 | 0.02 | 0.00 |
| Step 2 | ||||||
| Negative Interruption x Morality/Ethic | -0.10 | 0.18 | - 0.03 | -0.00 | 0.06 | -0.00 |
| Step 1 | ||||||
| Negative Interruption | 0.28 | 0.06 | 0.26* | 0.23 | 0.05 | 0.24* |
| Centrality of work | 0.06 | 0.04 | 0.07 | 0.09 | 0.04 | 0.12** |
| Step 2 | ||||||
| Negative Interruption x Centrality of work | 0.03 | 0.09 | 0.02 | -0.04 | 0.08 | -0.03 |
| Step 1 | ||||||
| Negative Interruption | 0.30 | 0.06 | 0.28* | 0.25 | 0.05 | 0.25* |
| Wasted time | 0.07 | 0.05 | 0.08 | 0.04 | 0.05 | 0.05 |
| Step 2 | ||||||
| Negative Interruption x wasted time | 0.00 | 0.11 | 0.00 | -0.19 | 0.10 | -0.11 |
| Step 1 | ||||||
| Positive Interruption | -0.03 | 0.05 | -0.03 | 0.00 | 0.05 | 0.00 |
| Leisure | -0.20 | 0.04 | -0.26* | -0.15 | 0.04 | -0.22* |
| Step 2 | ||||||
| Positive Interruption x Leisure | -0.01 | 0.07 | -0.00 | -0.07 | 0.07 | -0.06 |
| Step 1 | ||||||
| Positive Interruption | -0.09 | 0.05 | -0.09 | -0.03 | 0.05 | -0.04 |
| Self reliance | -0.11 | 0.04 | -0.13** | -0.00 | 0.04 | -0.00 |
| Step 2 | ||||||
| Positive Interruption x Self Reliance | -0.13 | 0.08 | -0.09 | -0.08 | 0.07 | -0.07 |
| Step 1 | ||||||
| Positive Interruption | -0.08 | 0.05 | -0.08 | -0.04 | 0.05 | -0.05 |
| Hard Work | -0.03 | 0.04 | -0.03 | 0.07 | 0.04 | 0.10 |
| Step 2 | ||||||
| Positive Interruption x Hard work | -0.09 | 0.08 | -0.06 | -0.19 | 0.07 | -0.15* |
| Step 1 | ||||||
| Positive Interruption | -0.05 | 0.05 | -0.06 | -0.02 | 0.05 | -0.02 |
| Delay of Gratification | 0.08 | 0.04 | 0.12** | 0.05 | 0.04 | 0.08 |
| Step 2 | ||||||
| Positive Interruption x Delay of Gratification | -0.20 | 0.08 | -0.14** | -0.04 | 0.07 | -0.03 |
| Step 1 | ||||||
| Positive Interruption | -0.09 | 0.05 | -0.09 | -0.04 | 0.05 | -0.05 |
| Morality/Ethic | 0.00 | 0.03 | 0.01 | -0.00 | 0.02 | -0.00 |
| Step 2 | ||||||
| Positive Interruption x Morality/Ethic | 0.12 | 0.05 | 0.12** | 0.10 | 0.05 | 0.12** |
| Step 1 | ||||||
| Positive Interruption | -0.08 | 0.05 | -0.08 | -0.02 | 0.05 | -0.02 |
| Centrality of work | 0.06 | 0.05 | 0.07 | 0.10 | 0.04 | 0.13** |
| Step 2 | ||||||
| Positive Interruption x Centrality of work | 0.05 | 0.08 | 0.04 | -0.04 | 0.07 | -0.03 |
| Step 1 | ||||||
| Positive Interruption | -0.07 | 0.05 | -0.07 | -0.02 | 0.05 | -0.03 |
| Wasted time | 0.02 | 0.05 | 0.02 | 0.02 | 0.05 | 0.03 |
| Step 2 | ||||||
| Positive Interruption x Wasted time | 0.00 | 0.08 | 0.00 | -0.05 | 0.07 | -0.04 |
*p < .01. **p < .05.
Moderators: Hard Work and Morality/Ethic on General Health and Wellbeing
In Step 2 of Table 2 there are significant interaction effects between hard work and positive appraisal of work interruption on GHQ (ß = -0.15, t = -2.63, p < .01). There was a significant interaction between morality/ethics and positive interruption (ß = 0.12, t = 2.07, p < .05) on GHQ. Graphical representations of the interactions are shown in Figure 1 (c) and (d). Figure 1c shows employees with a strong belief in hard work reported reduced psychological distress and more highly appraised positive interruptions compared to employees who endorsed a weak belief in hard work. Furthermore, employees with weak morality/ethics reported reduced discomfort and highly appraised positively work interruptions compared to those with strong morality/ethics (Figure 1d). Hypothesis 2 is supported, indicating two significant moderator effects as predictors on general health and wellbeing.
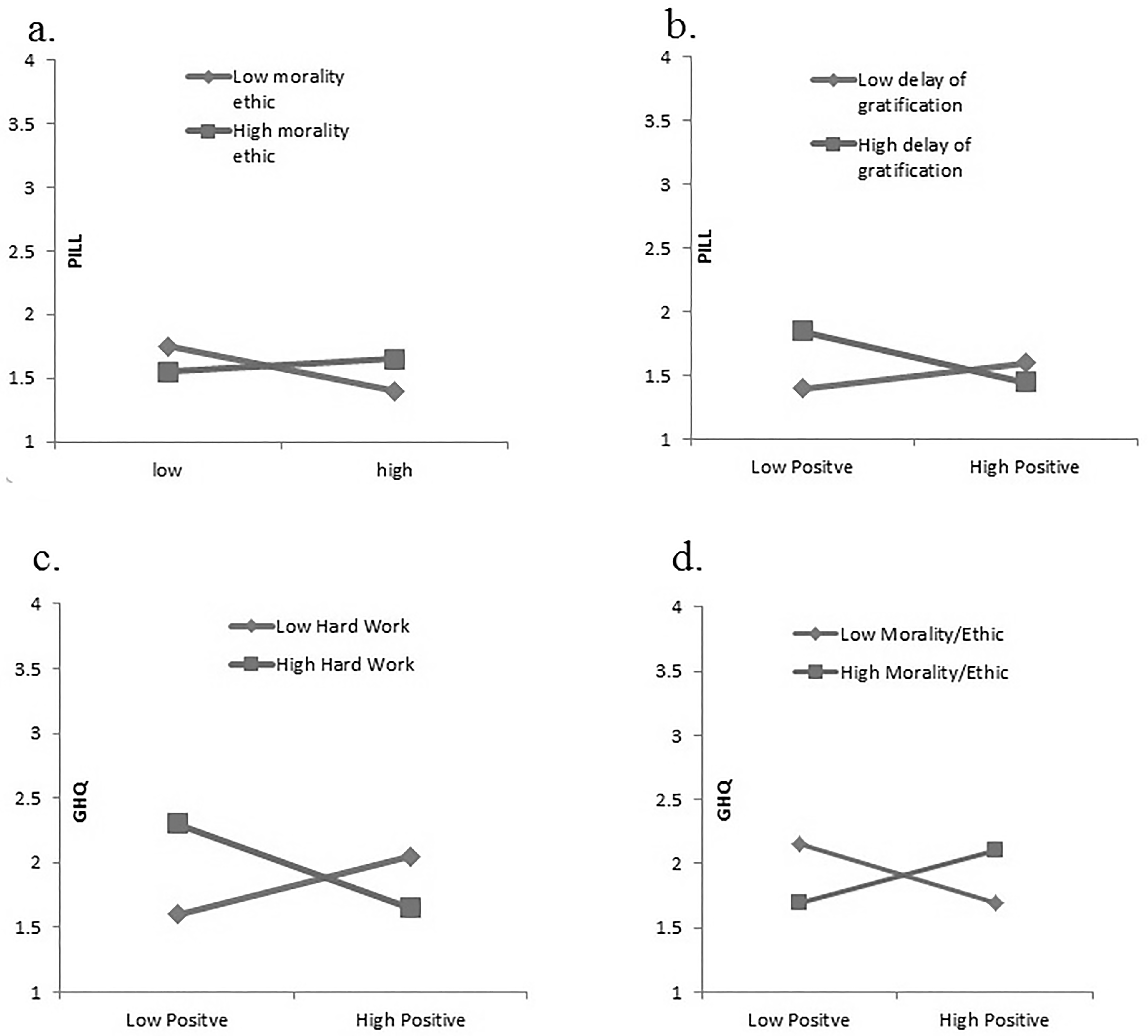
Figure 1
The Moderating role of work beliefs in the relationship between positive work interruption, wellbeing and general health.
Moderators: Delay of Gratification and Morality/Ethic on Psychosomatic Symptom
In Step 2 of Table 2, addition of the cross-product interaction terms to the regression equation (positive interruption x delay of gratification, positive interruption x morality/ethic) made a significant contribution to the prediction of physical complaints. Positive interruption and delay of gratification (ß = -0.14, t = -2.46, p < .05), and the effects of the interaction between positive interruption and morality/ethics (ß = 0.12, t = 2.17, p < .05) substantially contributed to psychosomatic symptoms. Graphical representations of the interactions are shown in Figure 1(a) and (b). Figure 1b shows reduced psychosomatic complaints for employees who reported a high belief in delay of gratification when they appraised highly positively work interruptions, compared to employees who endorsed a weak belief in delay of gratification. Moreover, employees who had a weak belief in morality/ethics when they appraised highly positively work interruptions reported low psychosomatic symptoms (see Figure 1a). Thus Hypothesis 3 was supported, indicating two significant moderator effects on psychosomatic symptoms. The interactions between positive appraisal of work interruptions and other work beliefs did not make any significant contribution to the prediction of psychosomatic symptoms (Table 2).
Discussion
Our results provided some support for the three general hypotheses underlying this study; work beliefs may serve as a link in the relationship between positive work interruption and general health and psychosomatic symptoms reports. In particular perceived job stress was associated with a negative attitude towards interruptions at the workplace. Age was negatively associated with physical health complaints and was positively associated with beliefs in hard work and leisure. Researchers found an increase in wellbeing among older employees compared to younger ones (Amati et al., 2010; Vandenberghe et al., 2011). One explanation could be that the experienced employees developed stress management techniques over time to better cope with work stressors (Mauno et al., 2013). Previous research has found that age adaption to stress improves over time, leading to a greater level of wellbeing (Isaacowitz & Blanchard-Fields, 2012; Staudinger & Kunzmann, 2005).
The correlation between age and positive attitudes towards interruptions is consistent with earlier research findings by Knights and McCabe (1998), highlighting that inexperienced employees at a bank demonstrated greater stress responses and sickness in comparison to experienced staff. Inexperienced staff conceived the “switching” from processing work to telephone calls as very difficult task, whereas the trained bank staff with prolonged years of experience in answering telephone calls perceived multi-tasking as an enjoyable and interesting experience. Therefore, the question arising is whether older employees could cope with work interruptions more effectively due to higher work experience.
The results support Hypothesis 1 thus illustrating those employees with strongly held positive belief in the importance of centrality of work and negative attitudes towards leisure have better health and wellbeing. These data are some of the first to describe the relationship between work beliefs, general and physical health. Consistent with previous findings (Hassall et al., 2005), the importance of belief in centrality of work and negative attitudes towards leisure were associated with improved psychological wellbeing. Employees who perceived work as important and meaningful had better psychological wellbeing (i.e. work reinforces self-esteem, provides financial reward and improves the quality of life). Also, employees who endorsed strongly held beliefs in work as a value were more likely to achieve a better wellbeing. Acknowledging this, it must be noted that the correlational nature of this type of research does not allow any causal association.
The results also support Hypothesis 2 suggesting that positive appraisal of work interruptions leads to reduced reports of distress, particularly when employees value the importance of hard work and do not hold the value of morality/ethics as important (disregard morality/ethics). These results are consistent with earlier research findings highlighting the important role of work beliefs related to improved general health (Hassall et al., 2005). Hassall et al. (2005) also supported the assumption that employees with strong beliefs in hard work and negative attitudes towards leisure demonstrated greater psychological wellbeing.
Furthermore, our results support the idea that some work beliefs moderate the relation between positive work interruption and psychosomatic symptoms as suggested in Hypothesis 3. More specifically, results showed that strongly held positive beliefs in delay of gratification and not holding the importance of morality/ethics as a belief become protective factors able to mitigate the effects of positive appraisal of work interruptions on psychosomatic symptoms. These beliefs affect the strength of the relation among positive appraisal of work interruption and psychosomatic work stress.
Overall there is a very small number of significant interaction effects; just four out of twenty-four interactions tested. Finally, the results of the present study showed that work beliefs did not moderate the relationship between negative attitudes towards work interruptions and psychosomatic complaints as well as between negative attitudes to work interruptions and general health and wellbeing. Previous research has argued that situational constraints including hassles due to interruptions at work can predict negative affect and proactive behaviour that brings change to an organization (Baethge & Rigotti, 2013; Sonnentag & Starzyk, 2015). In our study, it is likely that negative affect might influence employees’ negative attitudes to interruptions regardless of work beliefs which, in turn, influenced general health and psychosomatic complaints.
Implications
Intervention studies are needed to understand the role of work interruptions and the cognitive parameters of occupational wellbeing. Based on our findings, particular attention should be paid to employees’ workload and working hours when promoting occupational well-being; more specifically, employees assigned many responsibilities and are work interrupted have increased job demands and encounter an overload of tasks to be completed within limited time available during work hours. Hence, organizations need to develop action plans to cope with interruptions, and to also identify which work beliefs would be beneficial to promote occupational motivation and wellbeing. It is to be hoped that organizations will put in place suitable policies and incentives for developing a work ideology based on work beliefs and thus reinforce employees’ motivation. Supervisors could support employees in increasing their engagement by stimulating work beliefs with questions and explore how such changes impact on different levels of work performance. Previous research has shown that employees’ engagement was positively related to task performance (Christian, Garza, & Slaughter, 2011) and led to less fatigue during the working day (Sonnentag, Mojza, Demerouti, & Bakker, 2012).
In addition, the importance of work beliefs has implications for the theory of stress (Lazarus, 1996). Lazarus’ theory postulated that it is extremely important to analyse the role of cognitions or appraisals in the stress process, rather than only explore the objective environment. While cognitive factors have been recognized in occupational stress studies there has so far mainly been a focus on the negative consequences, for example of ruminating thoughts (Brosschot et al., 2006, 2014; Cropley & Zijlstra, 2011; Cropley et al., 2012). This study sheds light on how cognitive constructs and positive attitudes also may reduce the health impacts of work hassles. Consequently, a new look at the area of work beliefs as cognitions merits attention. Cognitive behavioural methods have been implemented with non-clinical samples as part of stress prevention training (van der Klink et al., 2001). Similarly, interventions focused on cognitive change have provided improvements in general health (Daniels, Harris, & Briner, 2002). The results of our study underscore the importance of looking at health in the workplace from perspectives such as these.
Limitations and Future Research Directions
This study used self-report measures, which are vulnerable to bias and can give rise to common method variance. However, the correlations observed were not so high as to suspect this was a major issue in the present study. One argument against a method of variance in the present study is that independent variables showed different relationships with dependent variables (delayed gratification positively correlated with physical complaints but not related with general health). The existing literature is also somewhat inconsistent as to what degree method variance can inflate the observed relationships among variables. A previous study found that an increase in variables entered in a regression, attenuated the effect of method variance on coefficients (Williams & Brown, 1994) leading to increased interaction effects (Williams & Brown, 1994). Similarly, Evans (1985) argued that method variance did not inflate product terms in moderated regression.
Future research could also conduct observational studies and interviews in which employees can describe positive work interruptions and its relation to work beliefs and physical symptoms. Future research should also assess whether work interruptions are associated with physiological parameters. The effort of being interrupted at work could cause an instant physiological reaction, such as a sharp rise in blood pressure and heart rate.
The 10-work interruption items questionnaire also emphasizes the role of subjective cognitions for work interruptions. Further studies with different samples are necessary to replicate the current findings and examine whether the items of the interruption questionnaire are invariant across occupations (managers, supervisors). Hinkin and Schriesheim (1989) argued that a “best practice” would occur if the measure was administered to an additional sample to assess the stability of the scale across time. For this purpose, the test-retest reliability of the measure needs to be examined. Moreover, further objective measures for work interruptions should be applied. Future research should consider phone calls, chats with colleagues and subordinates and attendance of meetings to evaluate the impact of different types of work interruptions on employees’ health indices.
Conclusion
This is the first study to examine the interrelationship between work interruptions, psychosomatic symptoms and general health. Interaction effects between the high appraisal of positive interruption and not holding the value of morality/ethics belief, as well as strong beliefs in delay of gratification emerged for reduced physical symptoms reports. The findings also suggest that beliefs in the importance of hard work and not have regard for morality serve as protective factors in the relationship between appraisal of positive interruption and improved general health and wellbeing.