 This is an open access article distributed under the terms of the Creative Commons
Attribution License (
This is an open access article distributed under the terms of the Creative Commons
Attribution License (Callous–unemotional (CU) traits were originally identified in an effort to define the heterogeneity of the population diagnosed with conduct disorder (CD) and antisocial personality disorder (ASPD) (Hill, 2003; Frick & Ellis, 1999). A lack of emotional valence and reduced empathy processing ability are key criteria for identifying these high CU trait subgroups (Guay, Ruscio, Knight, & Hare, 2007). Heterogeneous in nature, empathy is a psychological construct regulated by both cognitive and affective components (Feshbach, 1978). Cognitive empathy is the ability to attribute mental states to another given their environment and individual characteristics, whilst acknowledging that the individual’s mental processing may not be similar to one’s own; whereas, emotional empathy processes include both emotion recognition and emotion contagion (Blair, 2008, 2005). The congruency of both affective signals and higher cognitive inference is necessary to produce an empathetic response (Shamay-Tsoory, Aharon-Peretz, & Perry, 2009).
In clinical research, those with high CU traits typically present with an impairment of emotional empathy (Blair, 2005). For example, psychopathic participants are consistently less accurate at identifying fearful, sad, disgusted and happy facial affect (Blair, 2005; Hastings, Tangney, & Stuewig, 2008). Despite high CU trait clinical individuals manifesting disrupted emotional empathy processing, there is little evidence of an atypical cognitive empathic ability (Blair et al., 1996; Jones, Happé, Gilbert, Burnett, & Viding, 2010; Richell et al., 2003); however, Dadds et al. (2009) reported a dual deficit in cognitive and emotional empathy associated with high CU trait manifestation.
High CU trait clinical populations also present with reduced emotional reactivity, particularly to emotive stimuli which are negative in nature, such as those invoking anger, fear and pain (Loney, Frick, Clements, Ellis, & Kerlin, 2003). There is some evidence of reduced emotional reactivity to positive stimuli (Kimonis et al., 2008), although this association is not consistently reported (Verona, Patrick, Curtin, Bradley, & Lang, 2004).
CU traits are typically investigated in clinical populations; a paucity of research exists into the relationship between CU trait manifestation and the emotional and cognitive components of empathy processing, as well as emotional reactivity, in general populations. Edens, Marcus, Lilienfeld, and Poythress (2006) postulate that CU traits are normally distributed within this demographic; suggesting that, rather than there being a categorical dichotomy between clinical and general populations, CU traits may exist dimensionally across the two demographics.
The objective of the hereto within described research was to explore whether a similar pattern of empathy and emotional responding correlated with CU trait manifestation in the general population. It was predicted that a disruption in emotional empathy processing would be associated with higher levels of CU traits and that intact cognitive empathy ability would be probable at these same levels. It was also hypothesised that a reduced affective valence would be observed in response to negative emotional stimuli, and possibly, also to positive stimuli.
Method
Participants
In total, 124 participants completed the research tasks. The age range of the included participants was 18-45 years (M = 21.16, SD = 5.08). Of the recruited participants, 84 of the participants were female. A combination of students and graduates were included in the sample. None of the participants included in the data disclosed a history of high CU trait clinical disorders, such as Conduct Disorder or Antisocial Personality Disorder, during screening.
Materials
Self-Report Measures
CU trait manifestation and empathetic processing were scored using validated and commonly used self-report measures and an indirect measure of emotional valence. The Inventory of Callous–Unemotional Traits (ICU; Frick, 2004) is a 24-item questionnaire (e.g., “I do not show my emotions to others”) with responses given via a four point Likert scale ranging from 0 “Not at all true” to 3 “definitely true”; potential scores range from 0 to 72. Within the ICU, there are three subscales; these are uncaring, callousness and unemotional. An internal reliability of α = .73 has been demonstrated for the ICU (Kimonis et al., 2008).
The Empathy Quotient (EQ short-version; Baron-Cohen & Wheelwright, 2004) consists of 40 items (e.g. “I really enjoy caring for other people”), which the respondent rates on a four-point scale from ‘strongly agree’ to ‘strongly disagree’ An individual scores two points if they strongly agree, and one point if they slightly agree (e.g. each item is scored 2, 1, 0, 0); potential scores range from 0 to 80. Principal Components Analysis suggests a three-factor solution for the EQ: cognitive empathy, emotional reactivity (used as a measure of emotional empathy) and social skills (Berthoz, Wessa, Kedia, Wicker, & Grèzes, 2008; Lawrence, Shaw, Baker, Baron-Cohen, & David, 2004). Cronbach’s alphas have been observed for the EQ varying from .85 (Muncer & Ling, 2006) to .88 (Wakabayashi et al., 2006). The EQ has also been demonstrated to have good test–retest reliability (Lawrence et al., 2004). Furthermore, the EQ has established convergent validity with the Interpersonal Reactivity Index (IRI), the other self-report measure recruited for the described research (Lawrence et al., 2004).
The Interpersonal Reactivity Index (IRI; Davis, 1983) consists of 28 items (e.g. “I often have tender, concerned feelings for people less fortunate than me”) rated on a scale from A-E where A is scored as 0 and denotes ‘does not describe me well’ and E is scored as 4 and denotes ‘describes me very well’. Scores may range from 0-112. Within the IRI, four subfactors are assessed, these include; the perspective taking scale, the fantasy scale, the empathetic concern scale and, finally, the personal distress scale (Davis, 1983). The empathetic concern and perspective-taking subscales measure emotional and cognitive empathy respectively (Davis, 1983). Internal reliability as tested via Cronbach's alpha has been found to be good for the IRI (subscales range from α = .70 to α = .78); furthermore, the IRI measure demonstrated good test–retest reliability (subscales range from .62 to .81) (Davis, 1983).
Facial Expression Emotion Recognition and Response Task
Included in the task were 48 photographic stimuli which depicted the six basic emotions: happiness, fear, disgust, sadness, anger and pain. The images were selected after pilot testing found an agreement level of over 70% for each expression image; a level of agreement previously considered acceptable (e.g. Ebner, Riediger, & Lindenberger, 2010). Stimuli were portrait shots of individuals balanced for ethnic and gendered demographics. These were pseudo-randomly presented on a plain, light-coloured background. The Self-Assessment Manikin (SAM; Bradley & Lang, 1994) was used to record the participant’s emotional response to photographic stimuli in the emotional expression and emotional valence tasks. The SAM comprises two scales of five simple figures; these scales were labelled such that the design would test whether the participants felt negative or positive during their viewing of the stimuli and how intensely participants felt regarding the stimuli (Figure 1). The figures gave an additional pictorial cue to the scale to indicate valence or intensity.
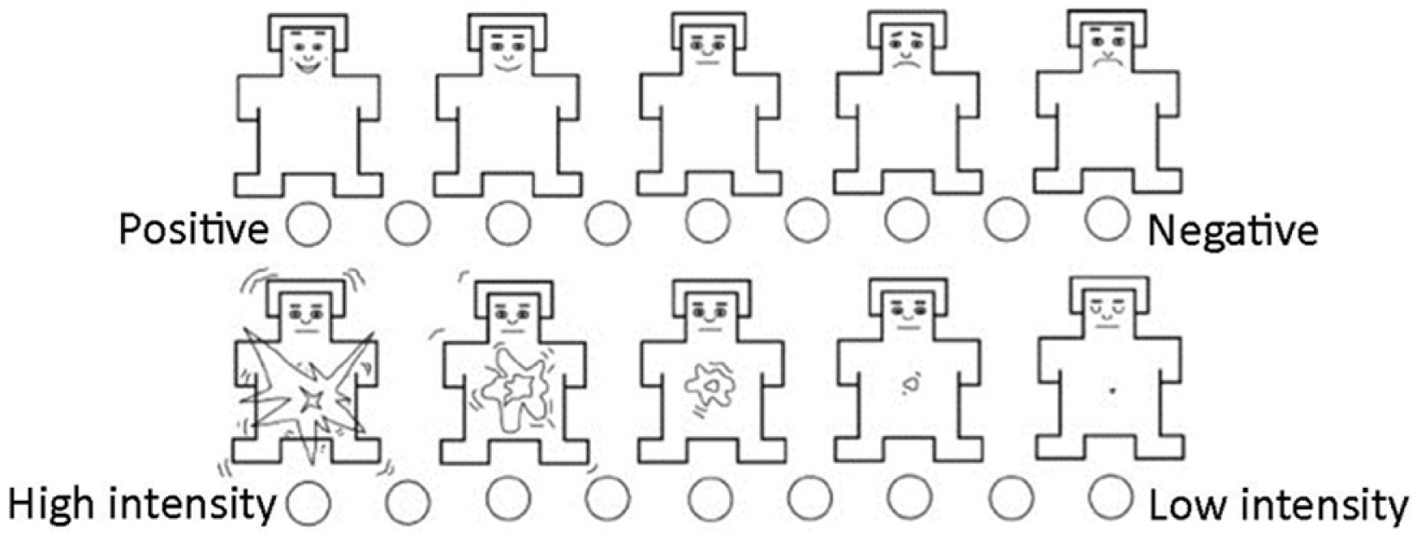
Figure 1
The adapted SAM (Bradley & Lang, 1994).
Affective Reactivity to Emotive Scenes Task
The emotional valence task investigated participants’ reactions to scenes containing emotional content. The emotional content consisted of 29 photographic stimuli from online sources, each photograph depicting a scene, which contained emotional subject matter. Stimuli were divided in to two distinct categories: those depicting positive and negative scenes, and stimuli concerning human and non-human subjects. The chosen stimuli included a total of 12 positive emotive scenes. Negative stimuli (specifically pain and fear) included a total of 17 photographic stimuli. Again, the SAM scales provide a measure of emotional reactivity.
Procedure
The self-report measures were presented via a PC, alongside clear instructions on how to complete the tasks. In addition to the self-report measures, the participants completed the facial expression recognition and response task, as well as the affective reactivity to emotive scenes task. For the emotional recognition task, the participants were required to note the emotion depicted using a drop down menu facility, which contained all six expressions as options. Participants completed the SAM scales to indicate how negatively/positively and how intensely they felt whilst viewing the stimuli. During the affective reactivity task, the participant rated the emotive scene stimuli on the two scales of the SAM in a manner that accurately reflected their own emotional experience. All tasks were completed in one testing session lasting up to 45 minutes.
Ethics
Participants were comprehensively briefed regarding their rights and the purpose of the study before giving their informed consent in line with APA guidelines. On completion of the data collection a debriefing procedure was completed.
Results
The descriptive statistics for the self-report measures of CU trait manifestation and empathy are given in Table 1.
Table 1
Descriptive Statistics for the Self-Report Measures of CU Traits and Empathy
| Measure | Subfactor [Possible Scores] | M | SD |
|---|---|---|---|
| Inventory of Callous - Unemotional Traits | Total [0-72] | 18.03 | 6.38 |
| Callousness [0-27] | 2.33 | 2.41 | |
| Uncaring [0-24] | 7.78 | 3.46 | |
| Unemotional [0-15] | 7.92 | 2.79 | |
| Empathy Quotient | Cognitive empathy [0-22] | 11.61 | 4.73 |
| Emotional reactivity [0-22] | 10.79 | 4.62 | |
| Interpersonal Reactivity Index | Perspective taking [0-28] | 17.64 | 4.63 |
| Empathic concern [0-28] | 20.06 | 4.60 |
Distribution and Reliability of the Callous-Unemotional Trait
The ICU total shows scores within the parameters of a normal distribution (see Figure 2). This is also true for two of the three ICU subscales; the uncaring and the unemotional subfactors. However, the callous subfactor revealed a positively skewed distribution (1.43). Internal reliability analysis with Cronbach’s Alpha shows appropriate internal reliability for the ICU total scores (24 items: α = .78). Cronbach’s alpha values above α ≥ .7 are commonly reported to be acceptable indicators of internal reliability (e.g., Dancey & Reidy, 2008). The unemotional subscale (5 items: α = .80) and uncaring subfactor (8 items: α = .73) showed good internal reliability, though the callousness subfactor (9 items: α = .62) was just outside this.
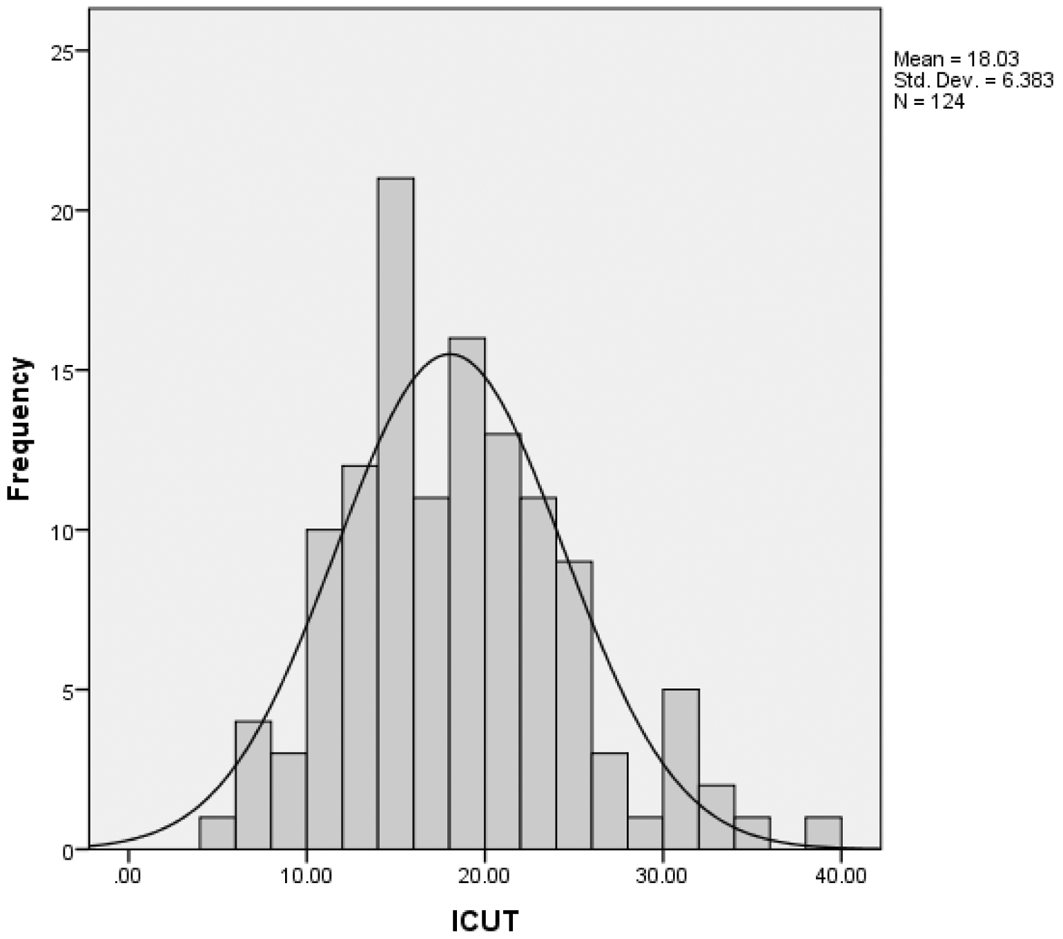
Figure 2
Distribution of CU trait scores on the ICU.
The results for the EQ and IRI lie within the necessary parameters to be considered a normal distribution. The internal reliability for the EQ cognitive empathy subscale (11 items: α = .85) and the emotional reactivity scale (11 items: α = .82) was good. When explored for internal reliability, both the IRI subfactors of empathetic concern (7 items: α = .77) and perspective taking (7 items: α = .79) were reliable.
An amalgamated score of the emotional empathy subfactors of the IRI and EQ were used to form a composite score for emotional empathy (M = 30.85, SD = 8.51); the same assimilation was performed to form the cognitive empathy measure (M = 29.25, SD = 7.16). The integrated emotional and cognitive empathy measures had a good level of internal reliability (18 items: α = .89 & 18 items: α = .81 respectively). The use of a composite score limited the reliance on any one measure and is argued to produce a more valid measure of each construct (Reniers, Corcoran, Drake, Shryane, & Völlm, 2011). The composite scores were within the parameters for normal distribution.
Correlations Between the Self-Report Measures of CU Traits and Empathy
The amalgamated, self-report measure of emotional empathy negatively correlated with scores on the ICU measure of CU traits (r(122) = -.66, p < .001), as did the self-reported cognitive empathy score (r(122) = -.51, p < .001). Finally, the association between emotional and cognitive empathy was significant (r(122) = .69, p < .001).
When gender is considered the expected differences are observed; females have higher mean scores in emotional and cognitive empathy, and males have higher CU trait scores (see Table 2 below). However, within the male and female groups, the negative relationship between CU traits and emotional and cognitive empathy was preserved (see Table 3 below).
Table 2
Differences in the Male and Female Scores on the Self-Report Measures of CU Traits and Empathy
| Measure | Mean
|
t-Test for Equality of Means
|
|||
|---|---|---|---|---|---|
| Female | Male | t | df | p | |
| CU Traits | 16.65 | 20.93 | -3.65 | 122 | <.001 |
| Emotional Empathy | 33.25 | 25.80 | 4.51 | 60.89 | <.001 |
| Cognitive Empathy | 30.72 | 26.15 | 3.47 | 122 | .001 |
Table 3
Correlations Between the Self-Report Measures of CU Traits and Empathy in Males and Females
| Gender | Emotional Empathy
|
Cognitive Empathy
|
||
|---|---|---|---|---|
| r | p | r | p | |
| Female | -.63 | <.001 | -.50 | <.001 |
| Male | -.59 | <.001 | -.40 | .005 |
Disassociation Between Emotional and Cognitive Empathy
A significantly stronger negative association was observed between the CU trait and emotional empathy coefficient, than for the CU trait and cognitive empathy coefficient (ZH = 2.13, p = .03). Dysfunction in emotional empathy is therefore correlated more strongly with higher CU trait manifestation, than deficiencies in cognitive empathy. Furthermore, using a standard multiple regression analysis the amount of variation in CU traits explained by the cognitive and emotional empathy predictors was found to be significant (F(2, 123) = 47.40, p < .001). The empathy predictors and CU traits were correlated at 0.663 with an adjusted multiple R2 of 0.43, indicating that 43% of the variation in CU trait scores could be predicted by empathy scores. Inspection of the regression coefficients and associated beta values revealed that only emotional empathy scores are a significant predictor of CU trait score (β = -.59, p < .001 (Tolerance = .52; VIF = 1.93)). Conversely, cognitive empathy was not a significant predictor of CU trait scores (β = -.095, p = .35 (Tolerance = .52; VIF = 1.93)).
Facial Emotion Recognition and Response
Analysis revealed that the ability to correctly identify negative facial expression stimuli (negative stimuli included depictions of disgust, fear, pain, anger and sadness) (M = 86.15%, SD = 8.92%) was significantly, positively associated with emotional empathy (r(122) = .25, p = .006) but did not correlate with levels of CU traits (r(122) = -.17, p = .065) nor the measure of cognitive empathy (r(122) = .15, p = .093). Considered individually, only correct identification of fearful expressions (M = 83.25%, SD = 18.09%) associated negatively with CU traits (r(122) = -.31, p = .001) and positively with emotional empathy (r(122) = .22, p = .015).
Analysis of the positive-negative valence scale of the SAM reveals that higher CU trait scores were associated with negative facial expressions being self-rated more positively (r(122) = -.24, p = .009). In addition, more negative scoring of negative facial expressions (M = 6.43, SD = .91) correlated with higher emotional empathy scores (r(122) = .40, p < .001); a pattern of scoring also observed for cognitive empathy (r(122)= .21, p = .018). This pattern of response was borne out over all 5 negative emotions. Higher CU trait scores were also correlated with more negative valence scores in response to happiness stimuli (r(122) = .39, p < .001), whereas, a higher score in emotional empathy or cognitive empathy was associated with more positive reports of experience to happiness stimuli (r(122) = -.44, p < .001 and r(122) = -.28, p = .001 respectively).
CU traits were associated with lower intensity to expressions of sadness and happiness (see Table 4). Higher emotional empathy was, however, associated with a global increase in emotional intensity to the combined negative emotions (r(122) = -.30, p < .001).
Table 4
Correlations Between the SAM Intensity Scores for Emotional Expressions and the Self-Report Measures of CU Traits and Empathy
| Emotion of Intensity Scored Expression | CU Traits
|
Cognitive Empathy
|
Emotional Empathy
|
|||
|---|---|---|---|---|---|---|
| r | p | r | p | r | p | |
| Happiness | .22 | .02 | -.18 | .04 | -.33 | < .001 |
| Sadness | .19 | .02 | -.24 | .003 | -.40 | < .001 |
Note. Lower scores indicate more intense responses.
Empathy Valence Task
The nine point positive-negative valence scale of the SAM (1 being the most positive score and 9 the most negative), observed that scoring higher on CU traits was associated with scoring less negatively on the scale when viewing negative images (r(122) = -.33, p < .001). Whereas, participants scoring highly on the measures of emotional empathy tended to score themselves as feeling more negatively when viewing the negative images (r(122) = .50, p < .001). This pattern of response was also observed for those higher in cognitive empathy (r(122) = .32, p < .001).
Higher CU trait score was associated with a pattern of response which indicated less positive affect in response to positive images (r(122) = .45, p < .001). Whereas, higher emotional empathy was associated with more positive scores for positive images (r(122) = -.50, p < .001); this pattern of correlation was also observed for measures of cognitive empathy (r(122) = -.41, p < .001).
Intensity of the participants’ feelings when observing the stimuli was reported using the SAM; a 1 on the scale indicated that a high intensity of emotion was experienced and a 9, low intensity. Those scoring highly on the CU trait measure tend to score themselves as experiencing less intensity of emotion when viewing both positive (r(122) = .18, p = .046) and negative (r(122) = .24, p = .008) images. Whereas higher emotional empathy was associated with increased intensity of affective valence for both positive (r(122) = -.27, p = .002) and negative (r(122) = -.47, p < .001) images. Cognitive empathy results mimic this pattern with smaller coefficients for both the positive (r(122) = -.19, p = .034) and negative (r(122) = -.27, p = .002) images.
Discussion
This study aimed to explore the relationship between CU traits, empathy processing and affective valence in a general population. Consideration of the ICU indirect measure of CU traits suggests that not only do CU traits manifest throughout the general population, measurement seems to suggest that CU traits present in a continuous distribution and within the parameters necessary to be considered normal. This finding is in agreement with previous research into CU traits (Edens et al., 2006). Therefore, disorders that are associated with the manifestation of high CU traits may represent the extreme high tail of this distribution, rather than being an isolated population of clinical high CU trait individuals.
Emotional empathy is evidenced to be dysfunctional within high CU traits clinical samples, however, cognitive empathy is usually reported intact (Blair, 2008, 2005). Despite this established empathy paradigm existing within the clinical populations, the results of this research into the general population did not evidence this same disassociation; suggesting instead that both emotional and cognitive empathy negatively correlated with CU traits. However, it is also revealed that the negative correlation observed between self-reported emotional empathy and CU traits is significantly larger than the corresponding CU trait correlation with cognitive empathy. Thus, the outcomes of the research suggest a difference in the magnitude of emotional and cognitive empathy processing reduction associated CU traits, rather than the clinical non-association of cognitive empathy with the reduced empathy processing being restricted to emotional empathy components.
The reduction in fear recognition accuracy associated with high CU traits demonstrated patterns of response concordant with clinical research, which has established a reliable dysfunction in the ability of those with high CU trait conditions to recognise fearful facial expressions (Blair, 2005; Hastings et al., 2008). No further reduction in recognition accuracy was observed; therefore, general population demographics may be specifically sensitive to modulation in fearful expression recognition with regards to CU trait manifestation.
Those high in CU traits consistently revealed a lower level of emotional intensity and valence in response to both positive and negative affective stimuli. This result mirrors the reduction in emotional responding evidenced in high CU trait disorders, such as psychopathy and conduct disorder, such disorders are associated with reduced empathetic response towards humans and sentient non-humans (Dadds, Whiting, & Hawes, 2006; Soderstrom, 2003). This pattern of negative association between emotional reactivity and CU traits, thus maybe a stable and permeating factor associated with CU trait manifestation.
To conclude, CU traits have been found to be present in a continuous distribution in the general population. Particularly, a lower reporting of both cognitive and emotional empathy is evidenced in those with higher CU traits. However, this finding lies counter to the disassociation of the construct processing associated with clinical populations. The deficit in affect recognition was not strongly evidenced in the results, with the exception of the fear condition. Deficiencies in emotional valence associated with elevated CU trait individuals were supported through indirect measurement of affect in the general population. As a constellation of results, the assimilated data suggests that CU traits are associated with modulations in both the empathy processing and affective reactivity in the general population.